Connections in the free part of the upper limb. The structure of man. Joints of the bones of the upper limb
text_fields
text_fields
arrow_upward
The scapula does not have direct contact with the bones of the body. It connects to them through the collarbone, which articulates with the sternum. But mainly the scapula is strengthened on the bones of the body with the help of muscles.
sternoclavicular joint
text_fields
text_fields
arrow_upward
sternoclavicular joint (articulatio stirnoclavicularis) formed by the medial end of the clavicle and the notch on the manubrium of the sternum.
The joint has a saddle shape, but allows movement in many axes, since there is a cartilaginous disk inside it. The bag of the joint is supported by ligaments heading to the 1st rib and to the clavicle of the other side.
At the lateral end, the clavicle forms a flat joint with the acromion and is connected by a ligament to the coracoid process. Both joints of the clavicle can be felt through the skin.
shoulder joint
text_fields
text_fields
arrow_upward
shoulder joint (articulatio humeri)- the most mobile joint of the body. It belongs to spherical multiaxial joints. The joint is formed by the head humerus and articular cavity of the scapula.
hollow significantly smaller head and is complemented along the edge with a cartilaginous lip. But even in this form, the area of \u200b\u200bthe cavity is only 1/4 of the area of \u200b\u200bthe articular head. This provides relatively free articular bag significant joint mobility, but reduces its strength.
From above, the joint is protected by a strong coracoacromial ligament, which forms above it, together with the shoulder process, the shoulder arch. The latter protects the joint but limits abduction and flexion of the arm. The bag fits freely around the joint and is supported only by a weak coracohumeral ligament.
The peculiarity of the joint is that the tendon of the biceps muscle of the shoulder passes through its cavity, covered in the region of the intertubercular groove with a synovial sheath, which facilitates its sliding. The tendon presses the head of the humerus against the cavity of the scapula.
In the joint, movements are possible along the axes: frontal (flexion and extension), sagittal (adduction and abduction) and vertical (outward and inward rotation), as well as circular movements (Fig. 1.24).
Rice. 1.24. Possible movements in the shoulder joint:
A - frontal axis: flexion-extension; B - sagittal axis: abduction-adduction; B - vertical axis: rotation
text_fields
text_fields
arrow_upward
elbow joint (articulatio cubiti) complex, as it combines three joints - humeroulnar, humeroradial And proximal radioulnar. They are surrounded by a common pouch, loose and relatively thin front and back, but reinforced by lateral ligaments. In addition, the neck radius held in the lunar notch ulna ring link.
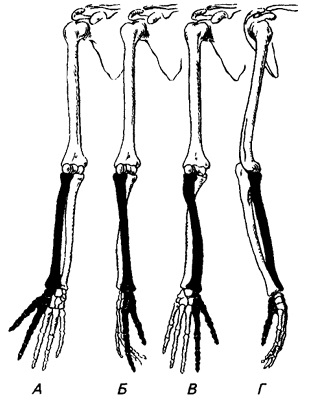 Rice. 1.25. Position of the hand and bones of the forearm
Rice. 1.25. Position of the hand and bones of the forearm In the humeroulnar and humeroradial joints, flexion and extension are possible, i.e. movement around the frontal axis.
In the cylindrical radioulnar joint, the radius rotates around vertical axis. In this case, rotation occurs in the spherical humeroradial joint.
The lower ends of the bones of the forearm form distal radioulnar joint, cylindrical in shape, combined with the proximal joint of the same name. Thanks to movements in these three joints, it is possible to turn the hand with the palm forward. (supination) and back (pronation), moreover, during supination, the bones of the forearm are set parallel to each other, and during pronation, the radius crosses the ulna (Fig. 1.25). The space between the bones of the forearm is tightened interosseous membrane.
A - with supination;
B - in the neutral position;
B - during pronation;
D - during rotation inward in the shoulder joint.
The radius and the corresponding part of the hand are black
wrist joint
text_fields
text_fields
arrow_upward
wrist joint (articulatio radiocarpea) formed by the distal end of the radius and three bones of the proximal row of the wrist (Fig. 1.26).
The pisiform bone is not involved in this joint. The joint is ellipsoid in shape: it can move along two axes - frontal (flexion and extension) and sagittal (abduction and adduction).
The ulna does not take part in this joint, since it is abducted from it by a triangular cartilaginous disk. The joint is strengthened by lateral (roundabout) ligaments originating on the styloid processes, as well as dorsal and palmar accessory ligaments.
Intercarpal joint
text_fields
text_fields
arrow_upward
Intercarpal joint (articulatio intercarpea) formed between the proximal and distal rows of the bones of the wrist, as a result of which its articular surfaces have complex outlines (Fig. 1.26). The bones that articulate here are connected by numerous short strong ligaments that limit the movements that occur along two axes.
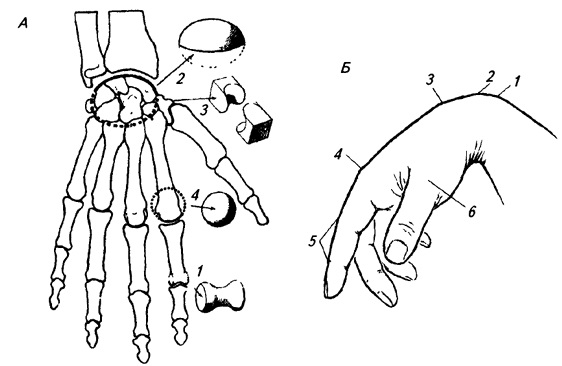 Rice. 1.26. Hand joints:
Rice. 1.26. Hand joints: A - joints of the hand: 1 - block-shaped; 2 - ellipsoid; 3 - saddle; 4 - spherical;
B - relief of the skeleton of a bent hand: 1 - head of the ulna; 2 - bones of the proximal row of the wrist; 3 - bases of the metacarpal bones; 4 - head II metacarpal bone; 5 - interphalangeal joints index finger; 6 - head of the I metacarpal bone
Mobility in this joint increases the movements of the hand that occur in the wrist joint. The bones in each row are interconnected by tight ligaments.
Carpometacarpal joints
Text_fields
arrow_upward
Metacarpophalangeal joints (articulationes metacarpophalangeae) spherical in shape (Fig. 1.26), but movements in them along the vertical axis are excluded by the ligamentous apparatus. In the thickness of the bursa of the I metacarpophalangeal joint, two sesamoid bones are included, protecting it from the palmar side.
Interphalangeal joints blocky, have lateral strengthening ligaments, movements in them are possible only around the frontal axis (Fig. 1.26).
Since many of the listed joints of the hand are located directly under the skin and are not covered by muscles, they largely form the back relief of the hand (Fig. 1.26, B).
Thus, during the evolution of man, the skeleton of the hand has undergone the following changes:
- phalanx bones thumb increased;
- the metacarpal-carpal joint of the thumb acquired a pronounced saddle shape;
- the thumb, as well as the large polygonal and navicular bones, have moved in the palmar direction;
- the phalanges of the II–V fingers shortened and straightened, which turned out to be very important for the development of fine differentiated hand movements.
Connections in the skeleton of the free part upper limb represented by the shoulder joint (articulatio humeri), the elbow joint (articulatio cubiti), the proximal and distal radioulnar joints (articulatio radioulnaris proximalis and articulatio radioulnaris distalis), the wrist joint (articulatio radiocarpea) and the joints of the skeleton of the hand - midcarpal, carpometacarpal, intermetacarpal, metacarpal but- phalangeal and interphalangeal joints.
The shoulder joint (Fig. 31, 32) is formed by the connection of the articular cavity of the scapula with the head of the humerus. The articular cavity of the scapula is surrounded by the articular lip (labrum glenoidale), which has a fibrocartilaginous structure. The articular lip increases the relatively small (compared with the head of the humerus) size of the articular cavity of the scapula, and also serves to absorb possible sudden movements in the joint.
The head of the humerus, in shape representing a third of the ball, provides greater joint mobility around all three axes, and also allows circular movements. The thickness of the cartilage covering the articular surfaces decreases from the center to the edges. The articular capsule, or bag (capsula articularis) (Fig. 31, 32), is attached to the scapula along the outer edge articular lip, and on the humerus along its anatomical neck, leaving the large and small tubercles of the humerus outside the joint cavity.
The joint capsule is strengthened by ligaments, which are thickened sections of its fibrous layer; highest value has a coraco-brachial ligament (lig. coracohumerale) (Fig. 32), passing from the base coracoid process. Most of its fibers are woven into the capsule, a smaller part reaches a large tubercle.
From the outside, in front and behind, the muscles and tendons of the muscles of the shoulder and shoulder girdle. From the bottom medial side the joint capsule does not have muscles that strengthen it, as a result of which there is a high probability of inferomedial dislocations in the joint.Synovial membrane joint (consisting of subsynovial and synovial layers) forms three inversions that expand the joint cavity. The largest of them - recessus axillaris - is located in lower section joint and is clearly visible when adducting the shoulder (Fig. 31).
elbow joint - compound joint, formed by the connection in the common capsule of the humerus with the ulna and radius.
There are three articulations in the elbow joint: humeroulnar, humeroradial, and proximal radioulnar.
The block-shaped humeroulnar joint is formed by the block of the humerus (Fig. 33, 34) and the block-shaped notch of the ulna (Fig. 33). The spherical humeroradial joint is made up of the head of the condyle of the humerus and the head of the radius (Fig. 34). The proximal radioulnar joint connects the articular circumference of the head of the radius with the radial notch of the ulna (see section "Bones of the forearm").
The shoulder joint provides flexion and extension of the arm at the elbow. The upper radioulnar joint of a cylindrical shape allows only rotational movements, that is, movements around the vertical axis - pronation and supination (in this case, the radius rotates along with the palm).
Fibrous fiber capsule elbow joint attached to the periosteum of the humerus in front of the radial and coronary fossae, behind the cubital fossa, in the lateral sections to the base of both epicondyles. On the bones of the forearm, the articular capsule is fixed along the edges of the articular cartilage on the ulna, and on the radius it is attached to its neck. Behind the capsule of the elbow joint is less strong.
The joint is strengthened by the radial (lig. collaterale radiale) and ulnar (lig. collaterale ulnare) collateral ligaments (Fig. 34, 35), which run from the epicondyles of the humerus to the ulna.
The proximal radioulnar joint is formed by the radial notch of the ulna, located on the lateral side of its upper epiphysis, and the head of the radius. The annular ligament of the radius (lig. annulare radii), attached to the ulna, covers the neck of the radius, thus fixing this connection.
The distal radioulnar joint (Fig. 36) is rotational, cylindrical in shape. The ulnar notch of the radius and the articular circumference of the head of the ulna that form it are separated by a triangular cartilaginous articular disc. The top of the disc is attached to the styloid process of the head of the ulna, and the base - to the ulnar notch of the radius. The joint provides adduction and abduction of the hand (its movement in sagittal plane).
The wrist joint (Fig. 36) is elliptical, connects the lower epiphysis of the radius and the articular disc (discus articularis) (Fig. 36) of the ulna with the bones of the proximal row of the wrist. Since the head of the ulna is at some distance from the wrist, free space filled with cartilage (fibrocartilago triangularis), which serves as the articular surface for the triangular bone. The carpal articular surface of the radius and the distal surface of the articular disc form the articular fossa wrist joint, and its head is the scaphoid, lunate and trihedral bones of the wrist. In about 40% of cases, the cartilage has a gap through which the radiocarpal joint can communicate with the lower radioulnar joint.
Movements in the joint occur around two axes: the hand can move in the sagittal plane (toward the radius or ulna), as well as bend and unbend, rotating around the frontal axis of the wrist joint.
The articular capsule is strengthened by the palmar radiocarpal ligament (lig. radiocarpale m. palmare), the radiocarpal ligament of the back of the hand (lig. radiocarpale m. dorsale), the ulnar and radial collateral ligaments (lig. collaterale carpi ulnare and lig. collaterale carpi radiale).
There are six types of joints in the hand: mid-carpal, inter-carpal, carpo-metacarpal, inter-metacarpal, metacarpophalangeal and interphalangeal joints (Fig. 37, 38).
The mid-carpal joint (articulatio mediocarpalis), which has an S-shaped joint space, separates the bones of the distal and proximal (except for the pisiform bone) rows of the wrist. The joint is functionally combined with the wrist joint and allows to slightly expand the degree of freedom of the latter. Movements in the mid-carpal joint occur around the same axes as in the wrist joint. Both joints are reinforced by the same ligaments.
Intercarpal joints (articulationes intercarpales) are interconnected side surfaces carpal bones of the distal row, and the connection is strengthened by the radiant ligament of the wrist (lig. carpi radiatum) (Fig. 38).
The carpometacarpal joints (articulationes carpometacarpales) connect the bases of the metacarpal bones to the bones of the distal row of the wrist. With the exception of the articulation of the trapezius bone with the metacarpal bone of the thumb (I) finger, all carpometacarpal joints are flat, their degree of mobility is small. The connection of the trapezoid and I metacarpal bones is trapezoid and provides significant mobility of the thumb. The carpometacarpal joint capsule is strengthened by the palmar and dorsal carpometacarpal ligaments (ligg. carpometacarpea palmaria et dorsalia) (Fig. 37, 38).
Intercarpal joints (articulationes intermetacarpales) are flat, with little mobility. They are formed by the lateral articular surfaces of the bases of the metacarpal bones (II-V), strengthened by the palmar and dorsal metacarpal ligaments (ligg. metacarpea palmaria et dorsalia) (Fig. 37, 38).
The metacarpophalangeal joints (articulationes metacarpophalangeales) (Fig. 37) are ellipsoid, connect the bases of the proximal phalanges and the heads of the corresponding metacarpal bones, are strengthened by collateral (lateral) ligaments (ligg. collateralia) (Fig. 37, 38). These joints allow movement around two axes - in the sagittal plane (abduction and adduction of the finger) and around the frontal axis (flexion-extension).
Interphalangeal joints (articulations interphalangeales) are block-shaped, connect the heads of the superior phalanges with the bases of the inferior ones. The interphalangeal joints provide flexion-extension of the fingers and are strengthened by collateral ligaments.
The heads of the metacarpal bones do not have an articular connection with each other; they are connected (on the palmar side) with a deep transverse metacarpal ligament (lig. metacarpeum transversum profundum) (Fig. 38).
The joints of the free upper limb connect the bones of this part to each other, as well as to the girdle of the upper limb. shoulder joint(articulatio humeri) is formed by the head of the humerus, the articular cavity of the scapula, which is complemented by the articular lip. The joint capsule covers the head of the humerus on the anatomical neck, and on the shoulder blade is attached along the edge of the articular cavity. The joint is strengthened by the coracobrachial ligament and muscles. The tendon of the long head of the biceps brachii passes through the joint cavity. The shoulder joint is a spherical joint in which movement is possible around three axes: frontal, sagittal and vertical. elbow joint(articulatio cubiti) - complex, it includes the humeroulnar, humeroradial and proximal radioulnar joints. These three joints have a common joint capsule, which is reinforced by the radial and ulnar collateral ligaments, as well as the annular ligament of the radius. The elbow joint belongs to the block-like joints: flexion, extension and rotation of the forearm are possible in it. Distal radioulnar joint(articulatio radioulnaris distalis) is an independent joint, and the proximal radioulnar joint is included in the elbow joint. However, they form a single combined cylindrical (rotational) joint. If the rotation of the radius occurs around the longitudinal axis along with the palmar surface of the hand inward, then such a movement is called pronation, and vice versa - supination. wrist joint(articulatio radiocarpalis) - a complex elliptical joint formed by the carpal articular surface of the radius and three bones of the first row of the wrist. Two types of movement are possible in it: adduction and abduction, flexion and extension, as well as a small passive circular movement. The joint is surrounded by a common capsule, it is strengthened by powerful ulnar, radial, palmar and dorsal radiocarpal ligaments. Hand joints include intermetacarpal, carpometacarpal, metacarpophalangeal, and interphalangeal joints. These joints are strengthened by short interosseous ligaments, which are located on the palmar and dorsal surfaces of the hand outside the joint cavities. The carpometacarpal joint of the thumb has a special structure. It is saddle-shaped in shape, it is characterized by two types of movement: flexion and extension, adduction and abduction, and possibly a circular movement, as well as opposing the thumb to the rest. The metacarpophalangeal joints are spherical, and the interphalangeal joints are block-shaped. The structural features of the bones and joints of the hand determine its extreme mobility, which allows you to perform very subtle and varied movements.
16. Bones of the pelvic girdle and their connection.
Belt lower limb(cingulum membri inferioris) consists of a paired pelvic bone. The pelvic bone, os coxae, refers to flat bones and performs the function of movement (participation in the joints with the sacrum and thigh), protection (of the pelvic organs) and support (transferring the weight of the entire overlying part of the body to the lower limbs). The latter function predominates, which determines the complex structure of the pelvic bone and its fusion from three separate bones - the ilium, os ilium, the pubis, os pubis, and the ischium, os ischii. Fusion of these bones occurs in the area the greatest load, namely in the region of the acetabulum, which is the articular fossa hip joint, in which the articulation of the belt of the lower limb with the free lower limb takes place.
The ilium lies above the acetabulum, the pubis lies downwards and anteriorly, and the ischium lies downwards and backwards. In persons under 16 years of age, the listed bones are separated from each other by cartilaginous layers, which ossify in an adult, i.e. synchondrosis turns into synostosis.
Thanks to this, out of three bones, one is obtained, which has a great strength necessary to support the entire body and head. The acetabulum, acetabulum (vinegar, from acetum - vinegar), is placed on the outside of the pelvic bone and serves to articulate with the head of the femur. Having the form of a rather deep rounded fossa, it is delimited along the circumference by a high edge, which is interrupted on its medial side by a notch, incisura acetabuli. articular smooth surface acetabulum has the shape of a crescent, facies lunata, while the center of the cavity, the so-called fossa acetabuli, and the part closest to the notch, are rough. Ilium
The ilium, os ilium, with its lower short thick section, called the body, corpus ossis ilii, merges with the rest of the pelvic bone in the region of the acetabulum; the upper, expanded and more or less thin part of it forms the wing of the ilium, ala ossis ilii. The relief of the bone is mainly due to the muscles, under the action of which ridges, lines and awns were formed in the places of the tendon method of attachment, and pits in the places of the fleshy attachment. So, the upper free edge of the wing is a thickened, S-curved crest, crista iliaca, to which three broad abdominal muscles are attached. The crest ends in front of the anterior superior spine, spina iliaca anterior superior, and behind it ends in the posterior superior spine, spina iliaca posterior superior. Below each of these awns, on the anterior and posterior margins of the wing, there is also an awn: spina iliaca anterior inferior and spina iliaca posterior inferior. The lower awns are separated from the upper notches. Below and anterior to the anterior lower spine, at the junction of the ilium with the pubic bone, is the iliopubic eminence, eminentia iliopubica, and downward from the posterior lower spine lies a deep large ischial notch, incisura ischiadica major, closing further down the ischial spine, spina ischiadica, located already on the ischium. The inner surface of the iliac wing is smooth, slightly concave and forms the iliac fossa, fossa iliaca, which arose in connection with the maintenance of the viscera in a vertical position of the body. Behind and downward from the latter lies the so-called ear-shaped articular surface, facies auricularis, the place of articulation with the sacral surface of the same name, and behind and upward from the articular surface is tuberosity, tuberositas iliaca, to which the interosseous sacroiliac ligaments are attached. The iliac fossa is separated from the inner surface of the underlying body of the ilium by an arcuate curved edge called the linea arcuata. On the outer surface of the wing of the ilium, more or less distinctly rough lines are visible - traces of attachments of the gluteal muscles (lineae gluteae anterior, posterior et inferior). Pubic bone
The pubic bone, os pubis, has a short thickened body, corpus ossis pubis, adjacent to the acetabulum, then the upper and lower branches, ramus superior and ramus inferior ossis pubis, located at an angle to each other. On the top of the angle facing the midline, there is an oval-shaped surface, facies symphysialis, a junction with the pubic bone of the other side. 2 cm lateral from this surface there is a small pubic tubercle, tuberculum pubicum, from which the pubic crest, pecten ossis pubis, extends along the posterior edge of the upper surface of the ramus superior, passing further posteriorly into the above-described linea arcuata of the ilium. On the lower surface of the upper branch pubic bone there is a groove, sulcus obturatorius, the passage of the obturator vessels and nerve. Ischium
The ischium, os ischii, like the pubis, has a body, corpus ossis ischii, which is part of the acetabulum, and a branch, ramus ossis ischii, forming an angle with each other, the apex of which is greatly thickened and is the so-called ischial tubercle, tuber ischiadicum. Along the posterior edge of the body, above ischial tuberosity, there is a small sciatic notch, incisura ischiadica minor, separated by the ischium, spina ischiadica, from a large sciatic notch, incisura ischiadica major. The branch of the ischium, moving away from the ischial tuberosity, then merges with the lower branch of the pubic bone. As a result, the pubic ischium their branches surround the obturator opening, foramen obturatum, which lies downward and medially from the acetabulum and has the shape of a triangle with rounded corners.
As a result, all types of connections are observed in the human pelvis, reflecting successive stages skeletal development: synarthrosis in the form of syndesmoses (ligaments), synchondroses (between separate parts of the pelvic bone) and synostoses (after their merger into pelvic bone), symphysis (pubic) and diarthrosis (sacral-iliac joint). The overall mobility between the bones of the pelvis is very small (4 - 10 degrees).
1. Sacroiliac joint, art. sacroiliaca, refers to the type of tight joints (amphiarthrosis), is formed by the ear-shaped articular surfaces of the sacrum and ilium in contact with each other. It is strengthened by ligg. sacroiliaca interossea, located in short bundles between the tuberositas iliaca and the sacrum, being one of the strongest ligaments of all human body. They serve as the axis around which the movements of the sacroiliac joint occur. The latter is also strengthened by other ligaments connecting the sacrum and ilium: front - ligg. sacroiliaca ventralia, behind - ligg. sacroiliaca dorsalia, as well as lig. iliolumbale, which extends from transverse process V lumbar vertebra to crista iliaca.
The sacroiliac joint is vascularized from aa. lumbalis, iliolumbalis et sacrales laterales. The outflow of venous blood occurs in the veins of the same name. The outflow of lymph is carried out through deep lymphatic vessels in nodi lymphatici sacrales et lumbales. The innervation of the joint is provided by branches of the lumbar and sacral plexuses.
2. The pubic symphysis, symphysis pubica, connects, located along the midline, both pubic bones to each other. Between the facies symphysialis of these bones facing each other, covered with a layer of hyaline cartilage, there is a fibrocartilaginous plate, discus interpubicus, in which, usually, starting from the age of 7, there is a narrow synovial gap (half-joint). The pubic symphysis is supported by a dense periosteum and ligaments; on the upper edge - lig. pubicum superius and on the lower - lig. arcuatum pubis; the latter smoothes the angle under the symphysis, angulus subpubicus.
3. Lig. sacrotuberale and lig. sacrospinale - two strong interosseous ligaments connecting the sacrum on each side with pelvic bone: the first - with tuber ischii, the second - with spina ischiadica.
The described ligaments complement the bony skeleton of the pelvis in its posterior-lower section and turn the large and small sciatic notches into openings of the same name: foramen ischiadicum majus et minus.
4. The obturator membrane, membrana obturatoria, is a fibrous plate covering the foramen obturatum of the pelvis, with the exception of the upper lateral angle of this opening.
Attached to the edges of the sulcus obturatorius of the pubic bone located here, it turns this groove into the canal of the same name, canalis obturatorius, due to the passage of the obturator vessels and nerve.
In the free part of the upper limb, the joints of the scapula, humerus, bones of the forearm and hand are isolated (Table 13).
shoulder joint(art. humeri) is formed by the articular cavity of the scapula and the head of the humerus (Fig. 100, 101). articular surface the head is spherical, almost 3 times the flat surface of the glenoid cavity of the scapula. The articular cavity is supplemented along the edges of the cartilaginous articular lip(labrum glenoidale), which increases the congruence of the articular surfaces and the capacity of the articular fossa. The articular capsule is attached to outside articular lip, as well as to the anatomical neck of the humerus. capsule shoulder joint thin, loose, loose. From above, the joint capsule is strengthened by the only one in this joint coracobrachial ligament(lig. coracohumerale), which begins at the base of the coracoid process of the scapula and is attached to the upper part of the anatomical neck of the humerus. The fibers of the tendons of adjacent muscles (subscapularis, etc.) are also woven into the capsule. The synovial membrane of the joint capsule forms two protrusions. One of them - intertubercular synovial sheath(vagina synovialis intertubercularis) like a case surrounds the tendon of the long head of the biceps muscle of the shoulder, passing through the articular cavity. The second protrusion - bursa of the subscapularis muscle(bursa subtendinea m. subscapularis) is located at the base of the coracoid process, under the tendon of this muscle.
The shape of the articular surfaces of the shoulder joint is spherical. It has a large range of motion around three axes, which is facilitated by a free joint capsule, a big difference in the size of the articulating surfaces, the absence of powerful ligaments. Flexion and extension are carried out around the frontal axis. The range of these movements in total is approximately 120°. Relatively sagittal axis abduction is performed (up to horizontal level) and cast hands. The range of motion is up to 100". With respect to the vertical axis, outward (supination) and inward (pronation) turns are possible with a total volume of up to 135 °. Circular movements (circumduxio) are also carried out in the shoulder joint. Movement of the upper limb above the horizontal level is performed in the sterno- clavicular joint when raising the scapula together with the free upper limb.
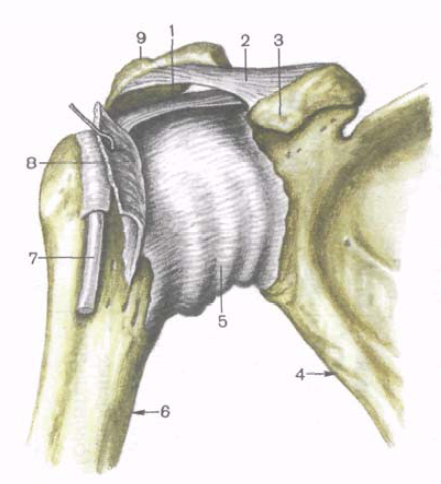
Rice. 100. Shoulder joint; front view. 1 - coraco-brachial ligament; 2 - coracoid-acromial ligament; 3 - coracoid process; 4 - scapula; 5 - joint capsule; 6 - humerus; 7 - tendon of the biceps muscle of the shoulder ( long head); 8 - tendon of the subscapularis muscle; 9 - acromion.
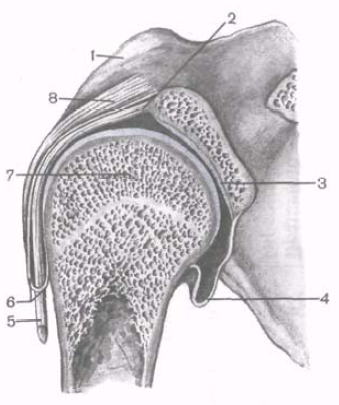
Rice. 101. Shoulder joint. (Saw in frontal plane.) 1 - coracoid process; 2.5 - tendon of the biceps muscle of the shoulder (long head); 3 - articular cavity; 4 - joint capsule; 6 - intertubercular synovial sheath; 7 - head of the humerus; 8 - coraco-brachial ligament.
On the radiograph of the shoulder joint (Fig. 102), the head of the humerus, the glenoid cavity of the scapula are clearly defined. The contours of the lower medial part of the head are layered on the glenoid cavity of the scapula. The X-ray slit in the picture looks like an arcuate strip.
elbow joint(art. cubiti) is formed by three bones: the humerus, radius and ulna (Fig. 103, 104). The bones form three joints enclosed in a common joint capsule.
Shoulder joint
(art. humeroulnaris) block-shaped, formed by the connection of the block of the humerus and the block-shaped notch of the ulna.
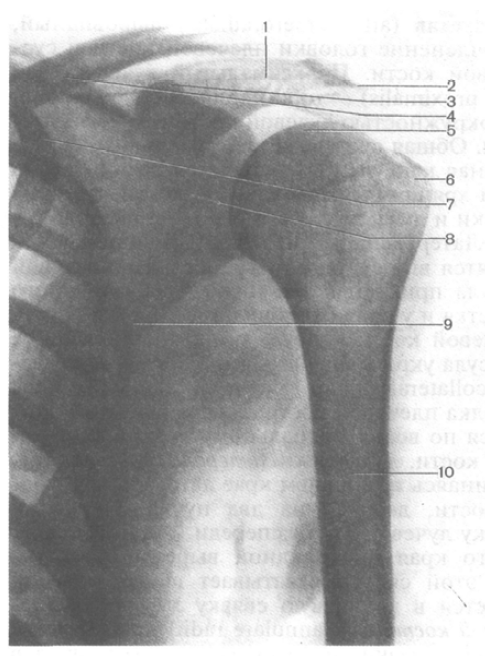
Rice. 102. X-ray of the shoulder joint, left. 1 - spine of the scapula; 2 - acromion; 3 - coracoid process; 4 - clavicle; 5 - head of the humerus; 6 - large tubercle (humerus); 7 - first rib; 8 - x-ray joint space; 9 - scapula; 10 - humerus.
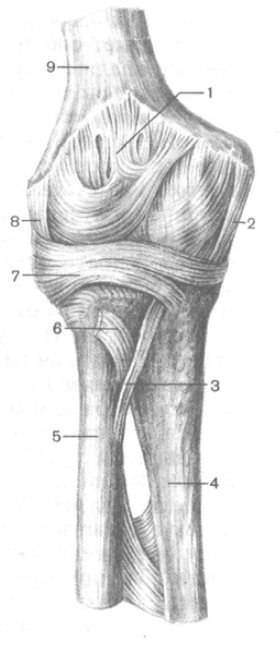
Rice. 103. Elbow joint; front view. 1 - joint capsule; 2 - ulnar collateral ligament; 3 - oblique chord; 4 - ulna; 5 - radius; 6 - tendon of the biceps muscle of the shoulder (cut off); 7 - annular ligament of the radius; 8 - radial collateral ligament; 9 - humerus.
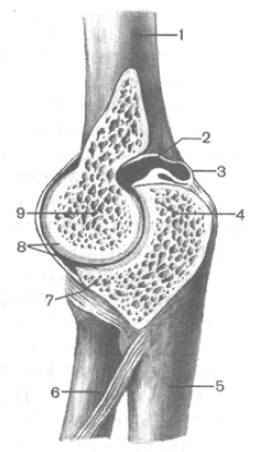
Rice. 104. Elbow joint. (Saw in the sagittal plane.) 1 - humerus; 2 - articular cavity; 3 - joint capsule; 4 - olecranon; 5 - ulna; 6 - radius; 7- coronoid process; 8 - articular cartilage; 9 - block of the humerus.
Shoulder joint(art. humeroradialis) spherical, represents the articulation of the head of the humerus and the articular cavity of the radius.
Proximal radioulnar joint (art. radioulnaris proximalis) - cylindrical in shape, formed by the articular circumference of the radius and the radial notch of the ulna. The common joint capsule is free. On the humerus, the articular capsule is attached relatively high above the articular cartilage of the humeral block, so the coronal and radial fossae and the olecranon fossa are located in the joint cavity. The lateral and medial epicondyles of the humerus are outside the articular cavity. On the ulna, the articular capsule is attached below the edge of the articular cartilage of the coronoid process and at the edge of the trochlear notch of the olecranon. On the radius, the capsule is attached to its neck. The joint capsule is reinforced with ligaments. Ulnar collateral ligament(lig. collaterale ulnare) originates below the edge of the medial epicondyle of the humerus, fan-shaped expands and is attached along the entire medial edge of the trochlear notch of the ulna. Radial collateral ligament(lig. collaterale radiale), starting at the lower edge of the lateral epicondyle of the humerus, is divided into two bundles. The anterior bundle covers the neck of the radius in front and is attached at the anterolateral edge of the trochlear notch of the ulna. Back beam This ligament covers the neck of the radius from behind and is woven into the annular ligament of the radius. Annular ligament of radius(lig. annulare radii) begins at the anterior edge of the radial notch of the ulna, covers the neck of the radius in the form of a loop and is attached at the posterior edge of the radial notch. Between the distal edge of the radial notch of the ulna and the neck of the radius is located square bundle(lig. quadratum).
In the elbow joint, movements around the frontal axis are possible - flexion and extension of the forearm with a total volume of up to 170 °. When flexing, the forearm deviates somewhat medially and the hand lies not on the shoulder, but on the chest. This is due to the presence of a notch on the block of the humerus, which contributes to the helical displacement of the forearm and hand. Around the longitudinal axis of the radius in the proximal radioulnar joint, the radius is rotated along with the hand. This movement occurs simultaneously in both the proximal and distal radioulnar joints.
When radiography of the elbow joint in the lateral projection (the forearm is bent at 90 °), the line of the x-ray joint space is limited by the trochlear notch of the ulna and the head of the radius on one side and the condyle of the humerus on the other. With a direct projection, the x-ray joint space is zigzag, has a thickness of 2-3 mm. The articular space of the proximal radioulnar joint is also visible.
Rice. 105. Connection of the bones of the forearm, right; front view. 1 - ulna; 2 - styloid process of the ulna; 3 - articular disc; 4 - styloid process of the radius; 5 - interosseous membrane of the forearm; 6 - radius; 7 - tendon of the biceps muscle of the shoulder; 8 - annular ligament of the radius.
The bones of the forearm are connected using discontinuous and continuous connections (Fig. 105). Continuous connection is interosseous membrane of the forearm(membrana interossea antebrachii).
It is a strong connective tissue membrane stretched between the interosseous edges of the radius and ulna. Down from the proximal radioulnar joint between both bones of the forearm, a fibrous cord is visible - oblique chord(chorda obliqua).
Discontinuous joints include the proximal radioulnar joint (discussed above) and the distal radioulnar joint, as well as the joints of the hand.
Distal radioulnar joint(art. radioulnaris distalis) is formed by the connection of the articular circumference of the ulna and the ulnar notch of the radius. This joint is separate from the wrist joint articular disc(discus articularis), located between the ulnar notch of the radius and the styloid process of the ulna. The articular capsule of the distal radioulnar joint is free, attached along the edge of the articular surfaces and the articular disc. The capsule usually protrudes proximally between the bones of the forearm, forming pouch(recessus sacciformis).
The proximal and distal radioulnar joints functionally together form a combined cylindrical joint with a longitudinal axis of rotation (along the forearm). In these joints, the radius, together with the hand, rotates around the ulna. In this case, the proximal epiphysis of the radius rotates in place, as the head of the radius is held by the annular ligament of the radius. The distal epiphysis of the radius describes an arc around the head of the radius, which remains motionless. The average range of rotation in the radioulnar joints (supination and pronation) is approximately 140°.
Joints of the bones of the girdle of the upper limb
1. Own bundles shoulder blades- these are two ligaments that are not related to the joints. The first of them - the coracoid-acromial - is the strongest ligament of the scapula, has the shape of a triangular plate, starts from the anterior edge of the apex of the acromial process and is widely attached to the coracoid process. It forms the “arch of the shoulder joint”, which protects the joint from above and limits the movement of the humerus in this direction.
The second - the upper transverse ligament of the scapula - is a short thin bundle thrown over the notch of the scapula. Together with the notch of the scapula, it forms an opening for the passage of blood vessels and nerves, and often ossifies.
2. Connections between the bones of the belt. Between the acromial process and the clavicle, the acromioclavicular joint (articulatio acromioclavicularis) is formed. Its articular surfaces are slightly curved, rarely flat. The joint capsule is tight, reinforced by the acromioclavicular ligament. Very rarely in this joint there is an intra-articular disc, which divides the joint cavity into two floors.
Movements in the acromioclavicular joint are possible in all directions, but their volume is insignificant. In addition to the aforementioned ligament, a strong coracoclavicular ligament prevents movement. It is divided into two ligaments: a quadrangular trapezoid, which lies laterally and anteriorly; and a narrower triangular conical, which is located more medially and posteriorly.
Both ligaments converge with each other at an angle open medially and anteriorly.
3. Connections between the bones of the girdle and the skeleton of the body. Between the clavicle and the handle of the sternum is the sternoclavicular joint (articulatio sternoclavicularis). Articulating surfaces are incongruent, covered with fibrous cartilage; their shape is very unstable, more often saddle-shaped. In the joint cavity there is an intra-articular disc that levels the articular surfaces of the bones, which do not correspond much to each other. The joint is saddle-shaped. The clavicle performs the most extensive movements around the sagittal axis - up and down; around the vertical axis - forward and backward. Circular motion is possible around these two axes. The articular capsule is reinforced by the anterior and posterior sternoclavicular ligaments, except for the lower surface, where the capsule is thin. These ligaments limit forward and backward movement.
In addition, the sternoclavicular joint is strengthened by the interclavicular and costoclavicular ligaments.
1 - articular disc; 2 - interclavicular ligament; 3 - anterior sternoclavicular ligament; 4 - clavicle; 5 - I rib; 6 - costoclavicular ligament; 7 - sternum
Of the bones of the shoulder girdle, only the clavicle is connected by its medial end to the skeleton of the body, so the bones of the girdle have great mobility; the movement of the scapula is directed and regulated by the clavicle, so the mechanical value of the latter is very large.
Joints of the free upper limb
This group includes the joints of the bones of the free upper limb with the girdle of the upper limb (scapula), as well as with each other.
The shoulder joint (articulatio humeri) is formed by the head of the humerus and the articular cavity of the scapula. The articular surface of the head of the humerus is one third (or slightly more) of the surface of the ball. The articular cavity has oval shape, slightly concave and in area is only a quarter of the surface of the head. It is complemented by an articular lip, which increases the congruence of the articulating surfaces, which are covered with hyaline cartilage.
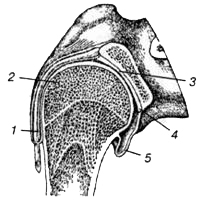
1 - tendon of the biceps muscle of the shoulder: 2 - head of the humerus; 3 - articular cavity of the scapula; 4 - articular lip; 5 - axillary bag
The articular capsule is very free, with a lowered limb it folds. It is attached on the scapula along the edge of the articular lip, and on the humerus along the anatomical neck, while both tubercles remain outside the joint cavity. Throwing in the form of a bridge over the intertubercular groove, the synovial layer of the joint capsule forms a blindly ending finger-like eversion - the intertubercular synovial sheath (vagina synovialis intertubercularis) 2-5 cm long. It lies in the intertubercular groove, covering the tendon of the long head of the biceps brachii, passing through the joint cavity above the head of the humerus.
The synovial membrane also forms a second permanent eversion - the subtendinous bag of the subscapularis muscle (bursa subtendinea m. subscapularis). It is located at the base of the coracoid process of the scapula, under the tendon of the subscapularis muscle and communicates widely with the joint cavity.
In the axillary cavity, the joint capsule becomes significantly thinner and forms a permanent deep fold in which the axillary synovial bursa(bursa synovialis axillaris).
The capsule of the shoulder joint is thin, strengthened from above and behind by the coraco-brachial and articular-shoulder ligaments.
- The coracobrachial ligament is well defined, starts from the base of the coracoid process and is woven into the capsule from the top and back. The direction of its fibers almost exactly coincides with the course of the tendon of the biceps muscle of the shoulder.
- The articular-shoulder ligaments are represented by three bundles, located above and in front, weaving into inner layer fibrous membrane of the articular capsule. They are fixed on the humerus to the anatomical neck and reach the articular lip.
The joint capsule, in addition to the ligaments, is strengthened by tendon fibers of the supraspinatus, infraspinatus, teres minor and subscapularis muscles. Consequently, the lower medial part of the capsule of the shoulder joint is the least strengthened.
The shoulder joint is typical spherical, multiaxial, the most mobile of all the discontinuous joints of the bones of the human body, since the articulating surfaces vary greatly in area, and the capsule is very spacious and elastic. Movement in the shoulder joint can be performed in all directions. Depending on the nature of the movements, the capsule relaxes, forms folds on one side and tightens on the opposite side.
The following movements are carried out in the shoulder joint:
- around the frontal axis - flexion and extension;
- around the sagittal axis - abduction to a horizontal level (further movement is prevented by the arch of the shoulder, formed by two processes of the scapula with the acromial-coracoid ligament thrown between them) and adduction;
- around the vertical axis - rotation of the shoulder in and out;
- when moving from one axis to another - a circular motion.
Movements around the frontal and sagittal axes are within 90°, rotation is somewhat less. Flexion, extension, abduction of the arm almost to the vertical, performed to the maximum extent, are carried out due to the mobility of the scapula and additional movements in the sternoclavicular joint.
Three bones are involved in the formation of the elbow joint (articulatio cubiti): the humerus, ulna and radius. Three simple joints are formed between them. All three joints have a common capsule and one articular cavity, therefore, from an anatomical and surgical point of view, they are combined into one (complex) joint. All articular surfaces are covered with hyaline cartilage.
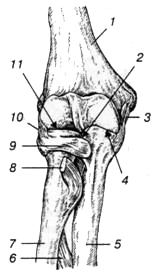
1 - humerus; 2 - proximal radioulnar joint; 3 - ulnar collateral ligament; 4 - shoulder joint; 5 - ulna; 6 - interosseous membrane of the forearm; 7 - radius; 8 - tendon of the biceps muscle of the shoulder; 9 - annular ligament of the radius; 10 - radial collateral ligament; 11 - shoulder joint
- Shoulder joint (articulatio humeroulnaris) formed by the articulation of the trochlea of the humerus and the trochlear notch of the ulna. The block of the humerus is a cylinder with a notch having a screw course. The joint is helical or cochlear in shape, uniaxial.
- Shoulder joint (articulatio humeroradialis) represents the articulation of the head of the condyle of the humerus with the articular fossa of the head of the radius. The joint is spherical in shape.
- Proximal radioulnar joint (articulatio radioulnaris proximalis) is a cylindrical joint and is formed by articulation upper ends radius and ulna.
All three joints are covered by one common joint capsule. On the humerus, the capsule is attached far from the edge of the articular cartilage: in front - 2 cm above the level of the epicondyles, so that the coronary fossa lies in the joint cavity. From the sides, the capsule is fixed along the border of the articular surface of the block and the head of the humerus, leaving the epicondyles free. The capsule is attached to the neck of the radius and along the edge of the articular cartilage of the ulna. Surrounding the articular semicircle of the radius, it thickens and forms an annular ligament that holds the proximal end of the radius. The capsule is thin anteriorly and posteriorly, especially in the region of the cubital fossa and at the neck of the radius.
In the lateral sections, the joint capsule is supported by strong collateral ligaments. The ulnar collateral ligament starts from the base of the medial epicondyle of the shoulder, diverges fan-shaped and attaches along the edge of the trochlear notch of the ulna. The radial collateral ligament starts from the lateral epicondyle of the shoulder, goes down and, without attaching to the radius, is divided into two beams. The superficial bundle of this ligament is closely intertwined with the extensor tendons, the deep one passes into the annular ligament of the radius, which, forming four-fifths of the circumference of the circle, covers the head of the radius from three sides (anterior, posterior and lateral).
The shoulder joint is spherical in shape, but in fact only two axes of motion can be used in it. The first axis runs along the length of the radius, coinciding with vertical axis proximal radioulnar joint - a typical cylindrical joint. Movement around this axis is performed by the radius together with the hand. The second axis coincides with the axis of the block (frontal axis), and the radius makes movements around it (flexion and extension) together with ulna. The glenohumeral joint functions like a helical joint (a type of trochlear joint). Lateral movements in the shoulder joint are completely absent, i.e., the sagittal axis in the joint cannot be realized due to the presence of an interosseous membrane and inextensible collateral ligaments between the bones of the forearm. The range of motion is approximately 140°. At the very strong flexion in the elbow joint, the coronoid process enters the coronary fossa, the forearm forms with the shoulder sharp corner(30-40°); at maximum extension, the humerus and the bones of the forearm lie almost on the same straight line, while the olecranon rests against the same-named fossa of the humerus.
Due to the fact that the axis of the humerus block runs obliquely with respect to the length of the shoulder, when flexed, the distal forearm deviates slightly to the medial side (the hand lies not on the shoulder joint, but on the chest).
The epiphyses of the ulna and radius are connected to each other by the proximal and distal radioulnar joints. Between the interosseous edges of these bones, a fibrous membrane (syndesmosis) is stretched, which is stronger in its middle section. It connects both bones of the forearm without interfering with movements in the proximal and distal radioulnar joints; part of the deep muscles of the forearm begins from it. Down from the proximal radioulnar joint, above the upper edge of the interosseous membrane, between both bones of the forearm, a fibrous bundle is stretched, called the oblique chord.
![]()
1 - proximal radioulnar joint; 2 - block notch of the ulna; 3 - oblique chord; 4 - ulna; 5 - distal radioulnar joint; 6 - triangular disk; 7 - carpal articular surface; 8 - radius; 9 - interosseous membrane of the forearm; 10 - tendon of the biceps muscle of the shoulder; 11 - annular ligament of the radius
As already noted, the proximal radioulnar joint is part of the elbow joint. The distal radioulnar joint is an independent joint, the shape of the articulating surfaces is similar to the proximal joint. However, in it the articular fossa is located on the radius, and the head belongs to the ulna and has a cylindrical shape. Between the lower edge of the ulnar notch of the radius and the styloid process of the radius is fibrous cartilage - the articular disc, which has the form of a triangular plate with slightly concave surfaces. It separates the distal radioulnar joint from the wrist joint and is a kind of articular fossa for the head of the ulna.
The proximal and distal radioulnar joints are anatomically independent, i.e., completely separate, but always function together, forming a combined rotational joint. Its axis in the extended position of the arm is a continuation of the vertical axis of the shoulder joint, constituting with it the so-called structural axis of the upper limb. This axis passes through the centers of the heads of the humerus, radius and ulna. The radius moves around it: its upper epiphysis rotates in place in two joints (in the humeroradial and proximal radioulnar,), the lower epiphysis describes an arc in the distal radioulnar joint around the head of the ulna. In this case, the ulna remains motionless. The rotation of the radius occurs simultaneously with the brush. Varieties of this movement are: outward rotation (supination) and inward rotation (pronation). Based on the anatomical stance, during supination, the hand turns with the palm anteriorly, the thumb is located laterally; during pronation, the palm turns back, the thumb is oriented medially.
The volume of rotation in the radioulnar joints is about 180°. If at the same time the shoulder and scapula make an excursion, then the hand can turn almost 360 °. The rotation of the radius is unimpeded in any position of the ulna: from the extended state to full flexion.
wrist joint
The wrist joint (articulatio radiocarpea) is formed by: the carpal articular surface of the radius, supplemented on the medial side by the articular disc, and the articular surfaces of the proximal row of carpal bones (ossa scaphoideum, lunatum et triquetrum). These bones of the wrist are firmly connected to each other by interosseous ligaments, therefore they form a single articular surface. This surface has an ellipsoidal shape and is much larger in area than the carpal articular surface of the radius.
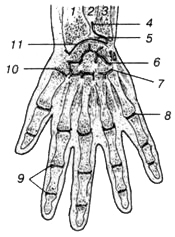
1 - radius; 2 - interosseous membrane of the forearm; 3 - ulna; 4 - distal radioulnar joint; 5 - triangular disk; 6 - mid-carpal joint; 7 - carpometacarpal joints; 8 - metacarpophalangeal joint; 9 - interphalangeal joints; 10 - metacarpophalangeal joint of the thumb; 11 - wrist joint
The articular disc is triangular in shape and separates the head of the ulna from the proximal row of carpal bones. In this regard, the ulna does not participate in the formation of the wrist joint. The joint capsule is attached along the edge of the articular surfaces. It is thin, especially at the back, but is complemented by ligaments on almost all sides. On the lateral side is the radial collateral ligament of the wrist, which starts from the styloid process of the radius and is attached to scaphoid. On the medial side is the ulnar collateral ligament of the wrist, which starts from the styloid process of the ulna and is attached to the triquetral and pisiform bones. On the palmar and dorsal surfaces of the wrist joint, there are, respectively, the palmar and dorsal wrist ligaments. The palmar ligament is thicker and stronger than the dorsal ligament.
In accordance with the classification of the bones of the hand, the following main joints are distinguished: between the bones of the proximal and distal rows of the wrist - the mid-carpal joint; between the bones of the distal row of the wrist and the bones of the metacarpus - carpometacarpal joints; between the bones of the metacarpus and proximal phalanges - metacarpophalangeal joints; between the proximal and middle, middle and distal phalanges - interphalangeal joints. These joints are reinforced by numerous ligaments.
Mid-carpal joint (articulatio mediocarpea) formed by the distal surfaces of the bones of the first row of the wrist (except for the pisiform) and the proximal surfaces of the bones of the second row of the wrist. The articulating surfaces of this joint have a complex configuration, and the joint space is S-shaped.
In this regard, the joint has, as it were, two spherical heads. Articulating articular surfaces are almost equal in area, therefore, in terms of range of motion, this joint is inactive. The articular capsule is attached along the edge of the articular surfaces, relatively free and very thin on the back. The joint capsule is strengthened by additional ligaments. The interosseous ligaments hold the bones of the distal carpal row very firmly to each other, so that movements between them are negligible. Between the bones of the second row of the wrist there are gaps connecting the cavities of the midcarpal and carpometacarpal joints.
Intercarpal joints (articulationes intercarpeae) are located between the individual bones of the proximal or distal rows of the wrist. They are formed by the surfaces of articulating bones facing each other, flat in shape. The cavities of these joints are narrow, communicating with the mid-carpal and carpometacarpal joints.
On the palmar and dorsal surfaces of the hand, there are numerous ligaments that connect the bones of the wrist, as well as the bones of the wrist with the bases of the metacarpal bones. They are especially well expressed on the palmar surface, making up a very strong ligamentous apparatus- radiant ligament of the wrist. This ligament originates from the capitate and radiates to the adjacent carpal bones. There are also palmar intercarpal ligaments that run from one wrist bone to another in a transverse direction. The complex of these ligaments lines the groove of the wrist and very firmly fastens the arch of the palm formed by the bones of the wrist and metacarpus. This vault is concave facing the palmar surface and is well expressed only in humans.
Above the groove of the wrist, between the radial and ulnar eminences of the wrist, there is a strong ligament - the flexor retinaculum (retinaculum flexorum), which is a thickening of the forearm's own fascia. The flexor retinaculum in the area of the specified elevation gives connective tissue septa to the bones of the wrist, as a result of which three separate canals are formed under it: the radial carpal canal, the carpal canal and the ulnar carpal canal.
Hand movements in relation to the forearm are performed around two mutually perpendicular axes: frontal and sagittal. Around the frontal axis there is a flexion of the hand, about 60-70°, and extension (about 45°). Around the sagittal axis, adduction (about 35-40 °) and abduction (about 20 °) are carried out. Thus, the range of motion during extension is much less than the range of motion during flexion, since extension is inhibited by well-defined palmar ligaments. Lateral movements are limited by the collateral ligaments and styloid processes. The hand also makes peripheral (conical) movements associated with the transition from one axis to another.
In all these movements, two joints take part - the wrist and middle wrist, which functionally make up one combined joint- joint of the hand (articulatio manus). The proximal row of carpal bones in this joint plays the role of a bone disc.
Quite apart from other articulations of the carpal bones is the pisiform joint (articulatio ossis pisiformis), which rarely communicates with the cavity of the wrist joint. The free capsule of this joint makes possible displacement bones in the distal-proximal direction.
Carpometacarpal joints (articulationes carpometacarpeae)- these are the joints of the bones of the distal row of the wrist with the bases of the five metacarpal bones. In this case, the joint of the thumb is isolated, and the remaining four joints have a common articular cavity and capsule. The articular capsule is tightly stretched, reinforced from the back and palmar sides by carpometacarpal ligaments. The joint cavity has a slit-like shape, located in the transverse direction. It communicates with the cavity of the midcarpal joint through the intercarpal joints.
II-V carpometacarpal joints in their form and function belong to the type of flat, inactive joints. Thus, all four bones of the second row of the wrist and the II-V metacarpal bones are very firmly connected to each other and mechanically constitute the solid base of the hand.
In the formation of the carpometacarpal joint of the 1st finger (articulatio carpometacarpea pollicis), the trapezoid bone and the 1st metacarpal bone take part, the articulating surfaces of which have a pronounced saddle shape. The joint capsule is free, from the palmar and especially from the back side it is strengthened by additional fibrous ligaments. The joint is anatomically and functionally isolated, movements in it are made around two mutually perpendicular axes: the sagittal one, passing through the base of the I metacarpal bone, and the frontal, passing through the trapezoid bone. In this case, the frontal axis is located at some angle to the frontal plane. Around it, flexion and extension of the thumb occurs along with the metacarpal bone. Since the axis of rotation runs at an angle to the structural axis of the upper limb, the thumb, when bent, shifts towards the palm, opposing the rest of the fingers. Around the sagittal axis, the thumb is abducted and adducted to the index finger. As a result of a combination of movements around the two named axes, circular motion is possible in the joint.
Joints of the bones of the fingers
Metacarpophalangeal joints (articulationes metacarpophalangeae) are formed by the heads of the metacarpal bones and the pits of the bases of the proximal phalanges. The articular surface of the heads of the metacarpal bones has a spherical shape, but from the sides it is cut off and extends more to the palmar surface. The articular cavity of the proximal phalanges is ellipsoidal and smaller. The joint capsule is free, thin, especially on the dorsal surface, and is supported by strong additional ligaments. On the medial and lateral sides of these joints, there are lateral ligaments that run from the pits on the lateral surfaces of the heads of the metacarpal bones to the tubercles at the bases of the proximal phalanges. From the palmar surface are even stronger palmar ligaments. Their fibers are intertwined with transverse bundles of the deep transverse metacarpal ligament. There are three last ligaments, they connect the heads of the II-V bones of the metacarpus, preventing their divergence to the sides and strengthening the solid base of the hand.
In shape, the metacarpophalangeal joints are spherical, except for the metacarpophalangeal joint of the thumb. Due to the large difference in the size of the articular surfaces of the heads and fossae, the joints have significant mobility, especially in the palmar direction. Around the frontal axis, flexion and extension up to 90 ° is performed in them, around the sagittal axis - the fingers are abducted to one side and the other (the total amount of movement of one finger is 45-50 °). Circular movements are also possible in these joints. Movement around the vertical axis in these joints is not realized due to the absence of rotatory muscles.
The metacarpophalangeal joint of the thumb (articulatio metacarpophalangea pollicis) is blocky in shape. The articular surface of the head of the I metacarpal bone is wide, on its palmar surface two tubercles are well expressed. The palmar part of the joint capsule includes two sesamoid bones (lateral and medial), one surface of which faces the joint cavity and is covered with hyaline cartilage. The amount of flexion in this joint is less than in II-V metacarpophalangeal joints.
The interphalangeal joints of the hand (articulationes interphalangeae manus) are located between the proximal and middle, middle and distal phalanges of the II-V fingers, as well as between the proximal and distal phalanges of the I finger. In education interphalangeal joints involved: the heads of the proximal or middle phalanges, which look like a regular block, and the bases of the middle or distal phalanges, represented by shallow pits with a ridge in the middle. The capsule of the interphalangeal joints is extensive, thin on the dorsal side, and strengthened on the rest by the palmar and lateral ligaments (the thumb sometimes has one sesamoid bone in it). Lateral ligaments completely exclude the possibility of lateral movements.
Interphalangeal joints are typical block-shaped. Movements in them are carried out only around a single frontal axis. In this case, flexion and extension of the phalanges occurs in the amount of 50-90 °.
Joint diseases
IN AND. Mazurov









